


Uterine Evaluation
Quick Takeaways
- Uterine evaluation checks the health of your uterus before or during IVF treatment.
- There are 5 main methods — from a basic pelvic exam to MRI — and your doctor will choose based on your situation.
- Abnormalities like fibroids, polyps, or a thin uterine lining can affect IVF success if left unaddressed.
- Most evaluations are done before your first IVF cycle to catch any issues early.
- Identifying and treating uterine problems before embryo transfer significantly improves implantation rates.
Uterine evaluation is a standard part of the IVF workup. Before embryos are transferred, your reproductive endocrinologist needs to confirm that your uterus is structurally healthy and that the lining can support implantation. Problems like fibroids, polyps, or scarring can interfere with a successful pregnancy — and most of them are treatable once identified.
Why Is Uterine Evaluation Important for IVF?
Contents
The uterus is where the embryo implants and develops. Even a perfect embryo can fail to implant if the uterine environment isn’t right. Uterine abnormalities are found in a significant percentage of IVF patients who have had repeated implantation failures — many of whom had no symptoms beforehand.
A uterine evaluation is typically done before your first IVF cycle and may be repeated if previous transfers haven’t worked. The findings directly affect your protocol — for example, if a polyp is found, it will usually be removed before proceeding with stimulation and transfer.
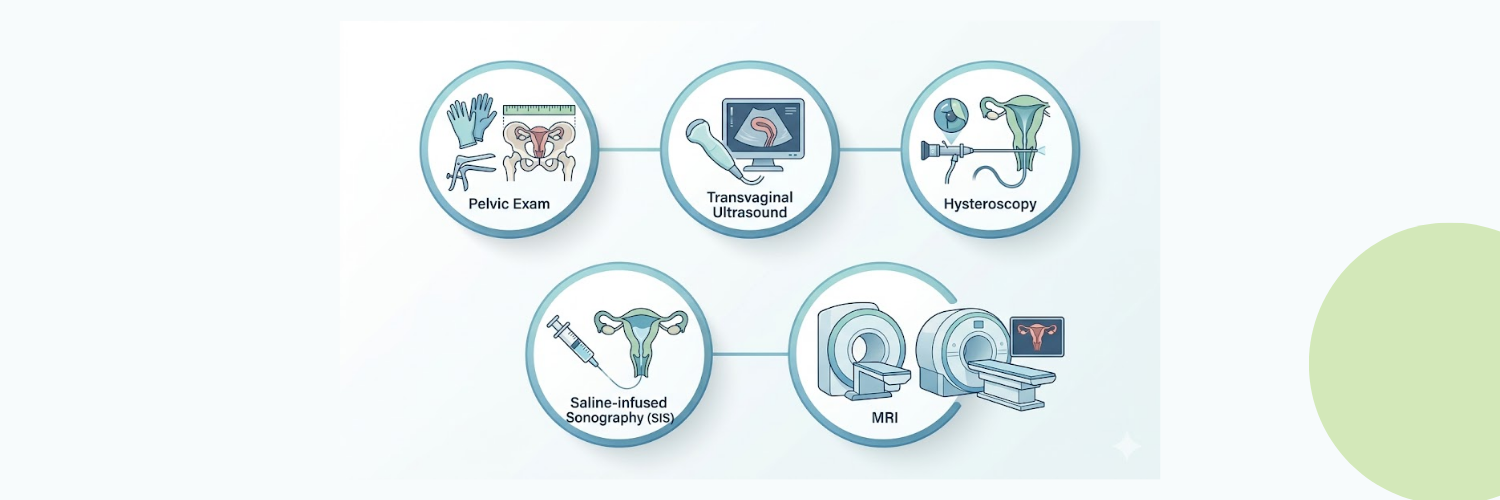
What Are the 5 Main Methods of Uterine Evaluation?
1. Pelvic Exam
A pelvic exam is the most basic starting point. Your doctor manually assesses the size, shape, and position of the uterus. While it can’t detect internal abnormalities like polyps or fibroids, it provides useful baseline information and helps identify things like an unusually tilted uterus that might affect catheter placement during embryo transfer.
2. Transvaginal Ultrasound
This is the most commonly used uterine evaluation tool in IVF. A small probe is inserted vaginally to produce high-resolution images of the uterus and ovaries. It measures the thickness and appearance of the endometrium (uterine lining), checks for fibroids or polyps, and assesses the ovarian antral follicle count — which helps predict how your ovaries will respond to IVF stimulation medications.
Transvaginal ultrasound is also used repeatedly throughout your stimulation cycle to monitor follicle growth in response to medications like Gonal-F or Menopur.
3. Hysteroscopy
Hysteroscopy involves passing a thin, lighted camera through the cervix directly into the uterine cavity. It gives the clearest possible view of the uterine lining and is the gold standard for diagnosing and treating abnormalities in the same procedure. Polyps, fibroids inside the cavity, adhesions (scar tissue), and septums can all be identified and often removed during the same session.
Many clinics recommend a diagnostic hysteroscopy before a first IVF cycle, particularly for patients with unexplained infertility or a history of miscarriage. It’s a short outpatient procedure done under light sedation.
4. Saline-Infused Sonography (SIS)
SIS — also called a sonohysterogram — involves injecting a small amount of sterile saline into the uterus while performing an ultrasound. The fluid separates the uterine walls and creates a much clearer picture of the cavity than a standard ultrasound alone. It’s particularly good at detecting polyps and submucosal fibroids that might be missed on a routine scan. SIS sits between a standard ultrasound and a full hysteroscopy in terms of invasiveness and detail.
5. MRI (Magnetic Resonance Imaging)
MRI isn’t used routinely in IVF workups, but it provides the most detailed structural imaging available when complex anatomy is suspected. It’s particularly useful for mapping the size and location of large fibroids, evaluating adenomyosis (a condition where uterine tissue grows into the muscle wall), or assessing congenital uterine anomalies like a bicornuate or septate uterus. Your doctor will order an MRI when ultrasound findings are inconclusive or when surgical planning is needed.
What Uterine Problems Can Affect IVF Success?
The most commonly found issues include:
- Endometrial polyps: Small tissue growths inside the uterine cavity. Usually benign but can interfere with implantation. Removed by hysteroscopy.
- Submucosal fibroids: Fibroids that grow into the uterine cavity. Associated with lower implantation and pregnancy rates. Often removed before IVF.
- Uterine adhesions (Asherman’s syndrome): Scar tissue inside the cavity, usually from a prior D&C or infection. Can be treated with hysteroscopic surgery.
- Thin endometrium: A lining under 7mm is generally considered too thin for transfer. Protocol adjustments — including estradiol supplementation — are used to thicken it.
- Uterine septum: A partial wall of tissue dividing the cavity. Associated with miscarriage risk. Treated surgically before transfer.
According to the American Society for Reproductive Medicine (ASRM), routine uterine cavity assessment before IVF is recommended for all patients, as undetected abnormalities are a common and correctable cause of implantation failure.
What Happens After a Uterine Evaluation?
If everything looks normal, you’ll proceed to ovarian stimulation — the phase where injectable FSH medications trigger your ovaries to develop multiple eggs. If an abnormality is found, treatment comes first, then IVF. Most uterine issues are straightforward to fix and don’t significantly delay your timeline.
Once you have a clear protocol, Fast IVF can supply all your stimulation and support medications at significantly lower prices than US retail. Browse the full product catalog or get a free price quote to see what you’d save on your cycle.
Frequently Asked Questions About Uterine Evaluation
Is uterine evaluation painful?
Most uterine evaluations involve minimal discomfort. A transvaginal ultrasound feels similar to a standard pelvic exam. SIS and hysteroscopy may cause brief cramping, similar to period pain, but are generally well-tolerated. Hysteroscopy under sedation causes no discomfort during the procedure. Your clinic will advise on what to expect before each test.
When in the cycle is uterine evaluation done?
Transvaginal ultrasounds are often done at the start of a cycle (day 2–5) to assess baseline uterine and ovarian status. SIS and hysteroscopy are typically scheduled in the first half of the cycle, before ovulation, when the uterine lining is thinner and the cavity is easier to visualize. Your clinic will time these tests around your natural cycle.
How does a thin uterine lining affect IVF?
Embryos need an endometrial lining of at least 7mm — ideally over 8mm — to implant successfully. A thin lining reduces implantation rates and may lead your doctor to cancel a transfer and freeze embryos for a later cycle. Estrogen supplementation, progesterone support, and other protocol adjustments are used to improve lining thickness in subsequent cycles.
Can fibroids always be removed before IVF?
Not always — it depends on the type and location. Submucosal fibroids (inside the cavity) almost always need removal before IVF. Intramural fibroids (within the muscle wall) are assessed case by case. Subserosal fibroids (on the outer wall) generally don’t affect the cavity and don’t require removal before transfer. Your doctor will decide based on size, number, and location.
What should I ask my doctor before my uterine evaluation?
Ask which evaluation method they recommend for your situation and why, whether any findings would delay your IVF cycle, and what treatment would look like if something is found. Also ask about timing — knowing which cycle day to schedule each test helps you plan around your work and medication schedule. Our FAQ & Policies page covers ordering and prescription questions once you’re ready to start your medication protocol.